
What is the anterior cruciate ligament (ACL)?
A ligament is a very strong and elastic band of connective tissue whose function is to connect bones within a joint. Specifically, knee stability is maintained by four ligaments: anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), and lateral collateral ligament (LCL).
From an anatomical point of view, the cruciate ligaments follow this path:
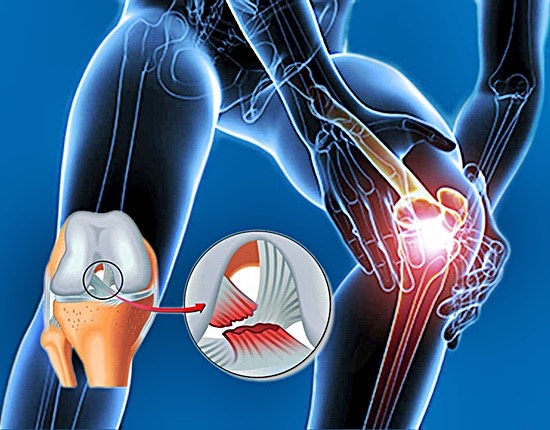
- Anterior cruciate ligament (ACL): It extends from the inner surface of the outer femoral condyle to the anterior intercondylar area of the tibia. Its function is to prevent the anterior displacement of the tibia relative to the femur. This ligament is where most injuries occur.
- Posterior cruciate ligament (PCL): It extends from the outer surface of the inner femoral condyle to the posterior intercondylar area of the tibia. Its function is to stabilize the posterior sliding of the tibia relative to the femur.
Depending on the degree of injury to the anterior cruciate ligament, they can be classified into three types:
- Grade I sprain: The ligament is slightly damaged, causing mild pain, swelling, and inflammation, with little or no functional impairment.
- Grade II sprain: Partial ligament tear, pain, swelling, and inflammation are greater, moderate functional impairment.
- Grade III sprain: Complete tear or rupture, pain, swelling, and inflammation are very intense, total functional impairment, and great knee instability.

Causes of anterior cruciate ligament injury
Most ACL injuries occur in sports activities that require lower limb turns and sudden stops:
- Quickly changing direction.
- Hyperextension with sudden knee rotation (rotating the knee with the ankle and foot firmly planted on the ground).
- Sudden stop.
- Direct trauma (direct contact or collision) to the back of the tibia.
- Combination of knee valgus (knee inward) and external rotation.
- Combination of knee varus (knee outward) and internal rotation.
- Incorrect landing.
- Decelerate the movement.
On the other hand, it is also important to highlight a series of risk factors that can increase the likelihood of suffering this injury:
- Playing sports such as soccer, basketball, alpine skiing, American football, etc.
- Being female: due to greater joint laxity (among other factors).
- Having poor physical condition.
- Excessive knee valgus.
- Playing sports on uneven terrain.
- Wearing inappropriate or oversized footwear.
Symptoms of anterior cruciate ligament tear
There are several pathologies with symptoms similar to those mentioned above when you injure your ACL (intense pain, swelling, edema, instability, discomfort when walking, etc.). To differentiate them, the following tests should be done a series of tests:
Drawer test
The injured person should lie supine (face up) with the hip flexed at 45° and the knee flexed at 90°. With the foot fixed in neutral rotation, healthcare personnel (doctor, physiotherapist, etc.) perform an anterior traction of the tibia. If a soft endpoint appears, there was an ACL injury.
X-ray
This test specifically will not clearly show the ACL injury, but it will show if it is associated with a bone injury.
MRI
This is one of the best tests to determine the degree of ACL injury since it creates better images of soft tissues.
Treatment of anterior cruciate ligament tear
Knee treatment in case of ACL injury will vary depending on whether it is conservative, that is, the affected person will not undergo surgery for their recovery, or if it is surgical. In general, most grade II and III tears usually opt for this form of treatment, especially when we are talking about athletes.
Non-surgical treatment
In case of conservative treatment, it is recommended strengthen the hamstrings (which can be worked on in an open kinetic chain) and quadriceps strengthening, taking into account that the load should be proximal to avoid favoring the anterior drawer. All these types of exercises should be prescribed by healthcare personnel (physiotherapist or doctor).
Surgical treatment
Regarding surgical treatment, it should be noted that the treatment used is ligamentoplasty, thus reconstructing the ligament, various materials can be used:
- Autograft (tendon graft): This is the most commonly used method. For this, fibers are taken from the patellar tendon or the pes anserinus tendon of the patient.
- Allografts: the tendon used for ligamentoplasty comes from a cadaver.
- Prosthesis.
Once surgery is performed and medical discharge is received, the injured person must follow a strict rehabilitation under the guidance of a physiotherapist who will apply different techniques for optimal knee recovery.
Among these techniques, the pressotherapy. During the first days, it would be advisable to use mode 2 of our SIZEN machine, which is indicated to drain excess fluid accumulated in the knee after surgery.
Once the patient gradually returns to sports activity, they may feel muscle overload due to lack of sports habit, so mode 3 or 4 is more recommended, with which the athlete will achieve rapid muscle recovery.
How to prevent anterior cruciate ligament injury?
Finally, we will give you a series of tips so you can prevent, as much as possible, anterior cruciate ligament injury, thus avoiding long months of sports inactivity:
- Strengthening of the hamstrings, quadriceps, and abdominal muscles.
- Strengthening of the external hip rotator muscles such as the gluteus medius, gluteus maximus, and tensor fasciae latae.
- Visit the physiotherapist regularly to avoid overload of the muscles mentioned above so they can function properly.
- Avoid muscle fatigue by using SIZEN pressotherapy.
- Train techniques for jumps, turns, stops, and accelerations.
- Respect rest days.
- Perform the exercises with appropriate footwear.
Author
Alicia Vicario, physiotherapist and creator of Fisiovik (IG: @fisiovik).
I studied Sports Science and Physical Activity and specialized in the Health branch. I worked in a physiotherapy clinic for years as a sports rehabilitation specialist until I finally decided to pursue physiotherapy.
Share:
Runner's Syndrome: What It Is and How to Cure It
What has happened to Alexia Putellas?